
Original Research
9 (
156-164
3
); 156-164
doi:
10.25259/APOS_25_2019
Effectiveness of low binding frictional materials: Evaluation of the binding frictional resistance of improved superelastic nickel-titanium alloy wires with different bracket combinations
1Private Practice, Fukui, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, Tokyo, Japan
2Departments of Orthodontic Science, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, Tokyo, Japan
3Departments of Advanced Biomaterials, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, Tokyo, Japan

Published: 2019-09-28,
Accepted: 2019-04-24,
Received: 2019-03-28
How to cite this article: Shima Y, Koyama A, Uo M, Ono T. Effectiveness of low binding frictional materials: Evaluation of the binding frictional resistance of improved superelastic nickel-titanium alloy wires with different bracket combinations. APOS Trends Orthod 2019;9(3):156-64.
Accepted: 2019-04-24,
Received: 2019-03-28
© 2019 Published by Scientific Scholar on behalf of APOS Trends in Orthodontics
Licence
This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
How to cite this article: Shima Y, Koyama A, Uo M, Ono T. Effectiveness of low binding frictional materials: Evaluation of the binding frictional resistance of improved superelastic nickel-titanium alloy wires with different bracket combinations. APOS Trends Orthod 2019;9(3):156-64.
Abstract
Introduction:
This study aimed to evaluate the binding frictional resistance of improved superelastic nickel- titanium alloy wires (ISW) with different bracket combinations and to verify the effectiveness of low binding frictional materials by applying them in orthodontic treatment.Materials and Methods:
Straight stainless steel wire (SSW; 0.016 × 0.022-inch) and straight ISW (0.016 × 0.022- inch) were set to each displaced bracket, and the tensile resistance load was measured. The maximum tensile resistance load was statistically compared using the Tukey test. For exemplification, we treated a typical extraction case of Angle Class I crowding malocclusion with lip protrusion using lower binding frictional materials, which were selected based on tensile test results.Results:
The SSW and metal bracket combination had the largest maximum tensile resistance load, and the ISW and metal slot-equipped plastic bracket combination had the smallest load (P < 0.01). In a patient treated using lower binding frictional materials, the active treatment period was 9 months. Satisfactory patient results were obtained without using reinforced anchorage.Conclusions:
Binding frictional resistance varies, depending on the archwire and bracket combination. In a multibracket appliance, selecting materials with as low a binding frictional resistance as possible may make a more effective treatment.Keywords
Binding friction
Materials
Improved superelastic nickel-titanium alloy wire
Extraction case
INTRODUCTION
Superelastic nickel-titanium (Ni-Ti) alloy has superior mechanical properties such as superelasticity, shape memory effect, high spring back property, and low stiffness,[1-4] and it has been widely used in clinical orthodontic treatment for >30 years. The load delivered from the superelastic Ni-Ti alloy wire is influenced by oral temperature changes: When the temperature changes during reverse transformation due to unloading, the load has a higher value than the initial load. The tendency of the load to increase depends on its stress hysteresis.[5,6] Furthermore, the appliance was improved so that it would deliver a more stable orthodontic force under changing oral temperatures, and an improved superelastic Ni-Ti alloy wire (ISW) with lower stress hysteresis was developed (L and H Titan; Tomy International, Tokyo, Japan).[7] Due to the characteristics of the ISW, three-dimensional tooth movement was possible during the early stage of treatment by incorporating bends that were formed using a heat-bending machine (SOARER-X; Tomy International).[8-12]However, the orthodontic force delivered from the archwire in the oral environment during orthodontic treatment is different from the bending properties; the orthodontic force is always changing due to friction with the bracket slot.[13-15] Friction is classified as “classical friction,” “binding friction,” and “notching friction.” Of these, binding friction has a great influence during various tooth movement patterns such as leveling and space closing.[16-18] The mechanical properties of the orthodontic wire and the bracket slot type greatly affect binding friction.[19-22] Due to its lower stress hysteresis and stiffness, the binding friction of the ISW is lower than that of other Ni-Ti wires.[23]
In this paper, we evaluated the binding frictional resistance of ISWs with different bracket combinations. We selected lower binding frictional materials, based on tensile test results, and exemplified the use of the materials in a typical extraction case.
MATERIALS AND METHODS
Ethical statement
The study was performed in accordance with the Declaration of Helsinki, and the treatment plan was approved by the director of Shima Orthodontic Office.Tensile test for the evaluation of binding friction
We conducted tensile tests to evaluate the binding frictional resistance between the different wire and bracket combinations. The testing materials were as follows: Metal slot-equipped plastic brackets [Figure 1a; IPASS II, Ortho-Dentaurum, Tokyo, Japan], different types of metal slot-equipped plastic brackets [Figure 1b; Clear bracket SL+, Dentsply-Sirona K. K., Tokyo, Japan], and metal brackets [Figure 1c; Metal bracket, Dentsply- Sirona K. K.]. All brackets were the standard type with a 0.018 × 0.025 – inch slot for the mandibular anterior teeth. We used a universal testing machine (EZ-SX; Shimadzu Corp., Kyoto, Japan) to measure the tensile resistance load [Figure 2a].
Close
Figure 1::
Magnified photographs of the materials used in the study. (a) IPASS II (Ortho-Dentaurum, Tokyo, Japan). (b) Clear bracket SL+ (Dentsply-Sirona K. K. Tokyo, Japan). (c) Metal bracket (Dentsply-Sirona).
Magnified photographs of the materials used in the study. (a) IPASS II (Ortho-Dentaurum, Tokyo, Japan). (b) Clear bracket SL+ (Dentsply-Sirona K. K. Tokyo, Japan). (c) Metal bracket (Dentsply-Sirona).

Close
Figure 2::
Materials and tensile test apparatus. (a) Tensile test apparatus. (b) The 0.018 × 0.025 – inch bended stainless steel wire for fixing brackets. (c) Brackets bonded on an acrylic plate. (d) Schematic drawing of the tensile test apparatus.
Materials and tensile test apparatus. (a) Tensile test apparatus. (b) The 0.018 × 0.025 – inch bended stainless steel wire for fixing brackets. (c) Brackets bonded on an acrylic plate. (d) Schematic drawing of the tensile test apparatus.
Treatment case
The patient was a woman, aged 22 years and 1 month, who presented with a chief complaint about her lateral profile protrusion and irregularity of maxillary anterior teeth. The lateral facial photograph shows protrusion of the upper and lower lips [Figure 3]. Pre-treatment dental casts revealed that the first molar relationship was Angle Class I on both sides [Figure 4].
Close
Figure 3::
Pre-treatment facial and intraoral photographs.
Pre-treatment facial and intraoral photographs.

Close
Figure 4::
Pre-treatment dental casts.
Pre-treatment dental casts.

Close
Figure 5::
Pre-treatment lateral and posteroanterior cephalometric and panoramic radiographs.
Pre-treatment lateral and posteroanterior cephalometric and panoramic radiographs.
RESULTS
Tensile test for the evaluation of binding friction
With the SSW, the average value of the maximum tensile resistance load in combination with IPASS II bracket was smallest at 1.04 N (106.0 gf), compared with the Clear bracket SL+ value (1.53 N [156.0 gf]), and the metal bracket had the largest value at 2.21 N (225.3 gf) [Figure 6]. There were significant differences between them. However, with the ISW, the IPASS II bracket had a significantly smaller value at 0.26 N (26.5 gf), compared with the Clear bracket SL+ (0.47 N [47.9 gf]) and the Metal bracket (0.51 N [52.0 gf]).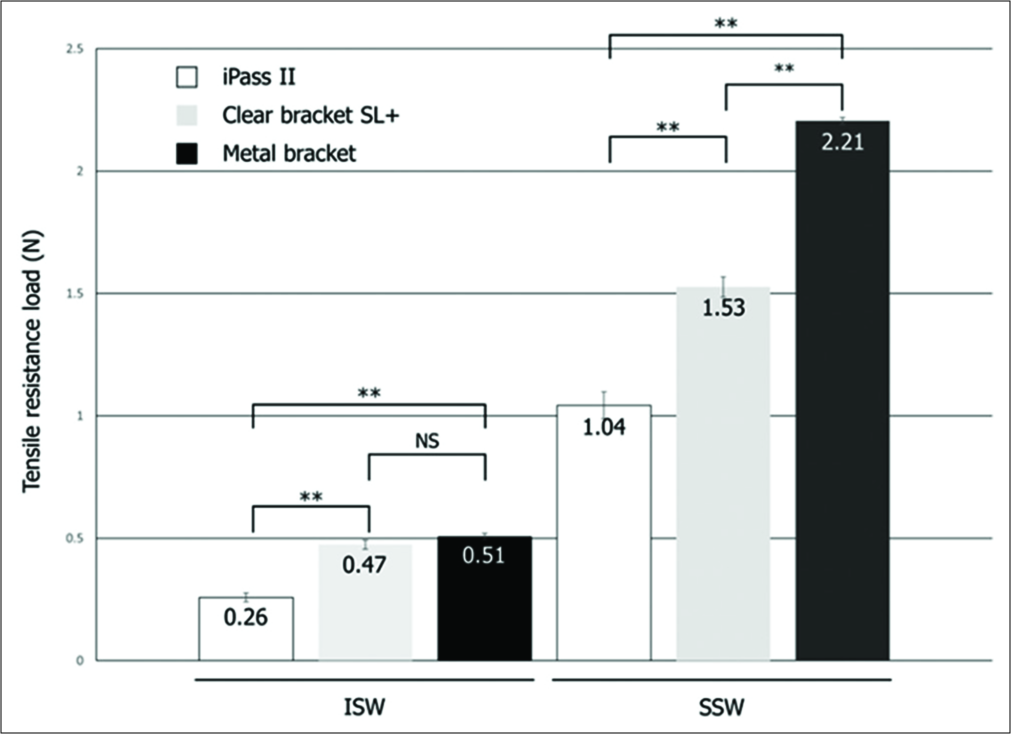
Close
Figure 6::
Results of the tensile test. **P < 0.01. ISW, improved superelastic nickel-titanium alloy wire; SSW, stainless steel wire.
Results of the tensile test. **P < 0.01. ISW, improved superelastic nickel-titanium alloy wire; SSW, stainless steel wire.
Treatment case
The intraoral photographs of the treatment progress at all patients’ visit are shown in Figures 7a-7i. After extracting the maxillary and mandibular first premolars, 0.018 × 0.025 – inch pre-adjusted IPASS II brackets were applied to the maxillary arch, and a 0.016 – inch Ni-Ti round wire (Sentalloy Blue; Tomy International) was applied as the initial archwire [Figure 7a]. In the following month, the same brackets were also applied to the mandibular arch and treatment was started with 0.016 × 0.022 – inch ISW [Figure 7b]. 2 months after beginning active treatment, a 0.016 × 0.022 – inch ISW was installed to the maxillary arch and space closure was continued [Figure 7c]. 3 months after initiating the active treatment, the use of the intermaxillary elastics (3/16 M; Tomy International) was initiated to improve the intermaxillary relationship [Figure 7d]. At the same time, the maxillary canine distalization was completed, and maxillary anterior retraction was initiated by sliding mechanics. Mandibular molar mesialization and lower anterior retraction were administered simultaneously. The maxillary and mandibular arches were treated using the same ISW wire until the end of the active treatment [Figures 7e-7i].
Close
Figure 7::
Intraoral changes in treatment progress. (a) At the start of active treatment. (b) 1 month later. (c) 2 months later. (d) 3 months later. (e) 4 months later. (f) 5 months later. (g) 6 months later. (h) 7 months later. (i) 8 months later.
Intraoral changes in treatment progress. (a) At the start of active treatment. (b) 1 month later. (c) 2 months later. (d) 3 months later. (e) 4 months later. (f) 5 months later. (g) 6 months later. (h) 7 months later. (i) 8 months later.

Close
Figure 8::
Post-treatment facial and intraoral photographs.
Post-treatment facial and intraoral photographs.

Close
Figure 9::
Post-treatment dental casts.
Post-treatment dental casts.

Close
Figure 10::
Post-treatment lateral and posteroanterior cephalometric and panoramic radiographs.
Post-treatment lateral and posteroanterior cephalometric and panoramic radiographs.

Close
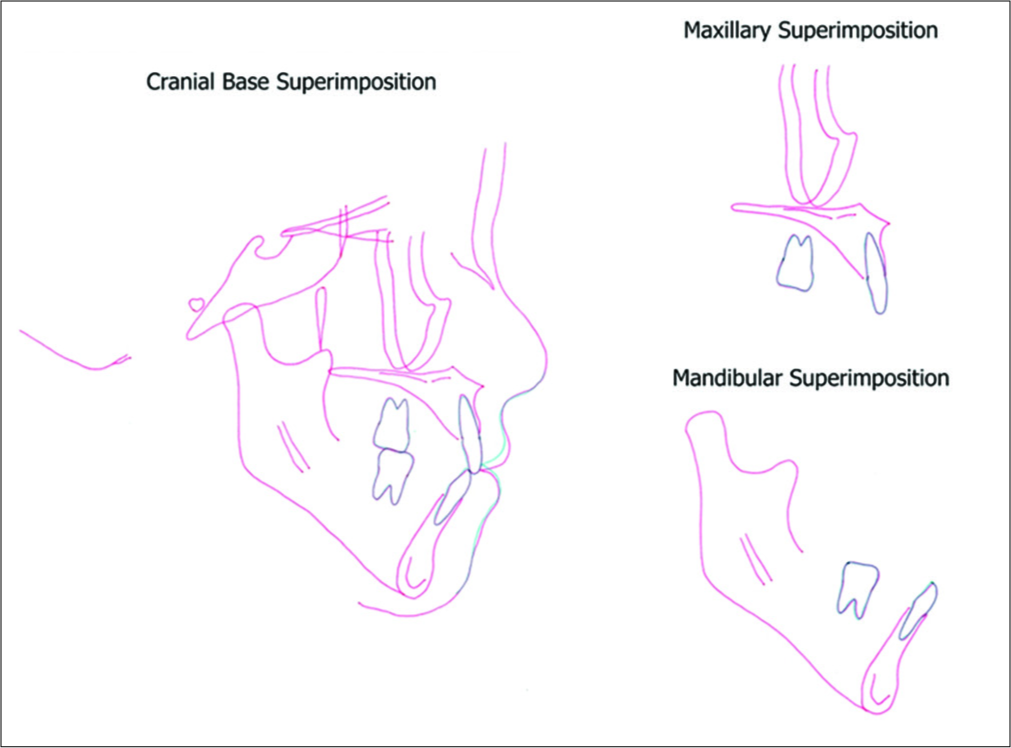
Figure 11::
Superimposed cephalometric tracings: Pre-treatment (black line) and post-treatment (red line).
Superimposed cephalometric tracings: Pre-treatment (black line) and post-treatment (red line).

Close
Figure 12::
Facial and intraoral photographs 2 years after treatment.
Facial and intraoral photographs 2 years after treatment.
Close
Figure 13::
Superimposed cephalometric tracings: Post-treatment (red line) and 2 years after treatment (green line).
Superimposed cephalometric tracings: Post-treatment (red line) and 2 years after treatment (green line).
Table 1:: Changes in cephalometric variables.
| Japanese norm | Pre-treatment | Post-treatment | |
|---|---|---|---|
| SNA (°) | 82.3±3.5 | 82.8 | 82.6 |
| SNB (°) | 78.9±3.5 | 77.7 | 76.8 |
| ANB (°) | 3.4±1.8 | 5.1 | 5.8 |
| FMA (°) | 28.8±5.2 | 37.8 | 38.0 |
| U-1–SN (°) | 104.5±5.6 | 113.1 | 99.1 |
| U-1–NP (mm) | 11.7±2.7 | 16.9 | 11.8 |
| IMPA (°) | 96.3±5.8 | 93.0 | 84.4 |
| Interincisal angle (°) | 124.1±7.6 | 109.0 | 131.2 |
FMA: Frankfort-mandibular plane angle
DISCUSSION
The efficiency of orthodontic tooth movement in a multibracket appliance is greatly affected by different types of friction generated between the archwire and the bracket slot.[13-20] With regard to friction classification, binding friction is generated by tipping the archwire in the bracket slot, which greatly affects tooth movement.[16] Movement occurs immediately after the wire bending exceeds the critical contact angle, and classical friction gives way to elastic binding at this point [Figure 14].[16,17] The critical contact angle depends on the materials and design of the wire and the bracket. Various studies[13-22,25-29] on binding friction have been reported. It is affected by the mechanical properties of the orthodontic archwire. Stiffer archwires exacerbate binding and then increase the frictional resistance between the archwire and the bracket slot.[20-22] In the comparison between different wire materials, Ni-Ti produced the least amount of friction.[19] As the angulation (and hence the binding) of the wire increases, there is a greater increase in frictional force with stainless steel than with Ni-Ti. This phenomenon is attributed to the excellent springback properties of Ni-Ti. Furthermore, based on one study,[23] which was conducted using Ni-Ti orthodontic wire products, ISW had a lower binding frictional resistance due to its lower stress hysteresis and stiffness, compared with conventional Ni-Ti wire (Sentalloy Yellow; Tomy International). Based on the findings in several reports,[19-23] the Ni-Ti round wire and ISW have lower binding frictional resistance. In particular, ISW has one of the least binding frictional resistances among various orthodontic wires.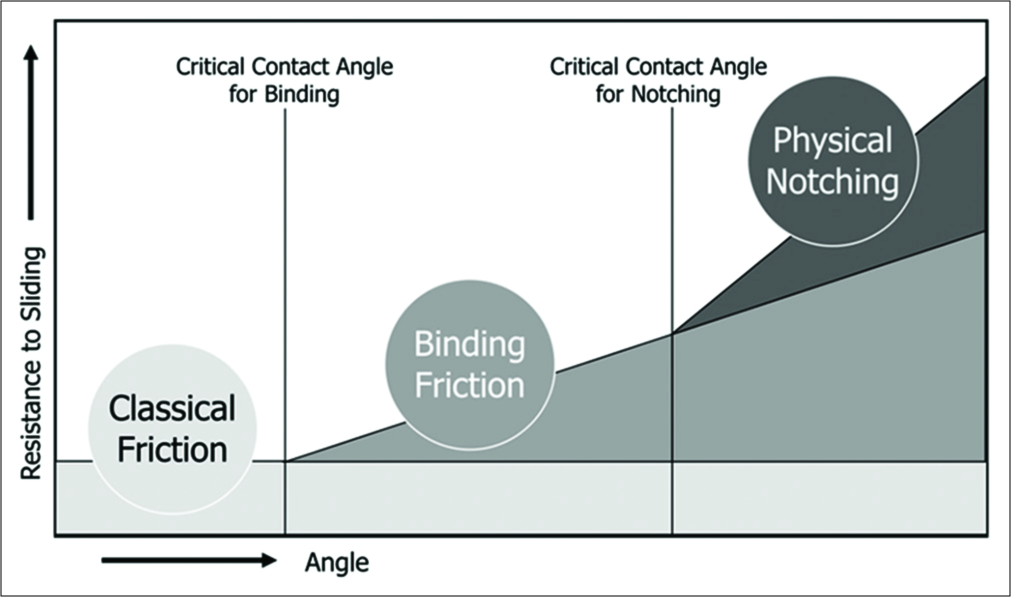
Close
Figure 14::
Friction classifications and the interrelationship between each classification.
Friction classifications and the interrelationship between each classification.
Binding friction in the vertical direction appears from the point where the wire tips and over the critical contact angle for binding in the bracket slot.[16,17] The mesiodistal opening of a general bracket slot is a right angle and the opening of the IPASS II bracket is an obtuse angle, although the critical contact angle for binding is larger and the binding friction may be smaller.
In the patient’s treatment, alignment was completed in approximately 2 months [Figure 7]. Alignment of the anterior teeth proceeded, along with canine distalization. Flare out of the maxillary anterior teeth was not observed. The anterior retraction was thereafter applied by sliding mechanics using the ISW, and space closure was nearly completed in 4 months. The low binding friction of the ISW combined with the IPASS II bracket seemed to work effectively during space closure.
The anchorage value of the maxillary molar was diagnosed as maximum. As described in the treatment objectives, we applied anchorage control using a light orthodontic force without reinforced anchorage devices. As a result, a possible reason for minimum (i.e., 1.0 mm) anchorage loss of the maxillary molar could be the low binding friction and the light orthodontic force. It is noteworthy that the superelasticity of the ISW is not only effective in the alignment, the ISW combined with the IPASS II bracket is but also effective, even in the space closure, due to the low frictional properties.
Based on the findings of this report, the combined use of the ISW and IPASS II bracket may reduce the binding frictional resistance. This reduction could contribute as one factor for more efficient orthodontic treatment in a short treatment period. However, the resistance to friction by binding examined in this report is a factor that should be considered clinically, and more detailed examination of the frictional behavior will be necessary with regard to the oral environment (e.g., under the wet condition).
CONCLUSIONS
- The ISW had low binding frictional resistance, which varied depending on different combinations of brackets.
- A successful treatment was possible using ISW with a lower binding frictional bracket in a typical extraction case.
- An effective treatment can be achieved by reducing the binding frictional resistance.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.Financial support and sponsorship
Nil.Conflicts of interest
There are no conflicts of interest.References
- Andreasen GF, Hilleman TB. An evaluation of 55 cobalt substituted nitinol wire for use in orthodontics. J Am Dent Assoc. 1971;82:1373-5
[CrossRef] [PubMed] [Google Scholar]
- Burstone CJ, Qin B, Morton JY. Chinese niTi wire a new orthodontic alloy. Am J Orthod. 1985;87:445-52
[CrossRef] [Google Scholar]
- Miura F, Mogi M, Ohura Y, Hamanaka H. The super-elastic property of the Japanese niTi alloy wire for use in orthodontics. Am J Orthod Dentofacial Orthop. 1986;90:1
[CrossRef] [Google Scholar]
- Miura F, Mogi M, Okamoto Y. New application of superelastic niTi rectangular wire. J Clin Orthod. 1990;24:544-8
[Google Scholar]
- Otsubo K, Yoneyama T, Hamanaka H, Soma K. Influence of temperature on the force level of a super-elastic NiTi alloy wire under strain. J Dent Mater. 1993;12:521-7
[Google Scholar]
- Otsubo K. Changes in force level of Ti-Ni alloy wires in the experimental oral environment. J Jpn Orthod Soc. 1994;3:55-61
[Google Scholar]
- Otsubo K. Development of the super-elastic Ti-Ni alloy wire appropriate to the oral environment. J Jpn Orthod Soc. 1994;53:641-50
[Google Scholar]
- Horiuchi Y, Horiuchi M, Soma K. Treatment of severe class II division 1 deep overbite malocclusion without extractions in an adult. Am J Orthod Dentofacial Orthop. 2008;133:S121-9
[CrossRef] [PubMed] [Google Scholar]
- Otsubo K, Imai N, Winarakwong L. Application of all-NiTi mechanics combined with J-hook headgear in the treatment of an adult high angle Class I extraction case. O J Thai Assoc Orthod. 2011;1:33-9
[Google Scholar]
- Ishida T, Yoon HS, Ono T. Asymmetrical distalization of maxillary molars with zygomatic anchorage, improved superelastic nickel-titanium alloy wires, and open-coil springs. Am J Orthod Dentofacial Orthop. 2013;144:583-93
[CrossRef] [PubMed] [Google Scholar]
- Ishida T, Ono T. Asymmetric severe skeletal class II division 1 patient with temporomandibular joint disorder treated with zygomatic anchorage devices and ni-ti alloy wires. Angle Orthod. 2014;84:919-30
[CrossRef] [PubMed] [Google Scholar]
- Ikeda Y, Kokai S, Ono T. A patient with mandibular deviation and 3 mandibular incisors treated with asymmetrically bent improved superelastic nickel-titanium alloy wires. Am J Orthod Dentofacial Orthop. 2018;153:131-43
[CrossRef] [PubMed] [Google Scholar]
- Frank CA, Nikolai RJ. A comparative study of frictional resistances between orthodontic bracket and arch wire. Am J Orthod. 1980;78:593-609
[CrossRef] [Google Scholar]
- Noda T, Okamoto Y, Hamanaka H. Frictional property of orthodontic wires evaluation by static frictional coefficients. J Jpn Orthod Soc. 1993;52:154-60
[Google Scholar]
- Noda T, Soma K. Frictional property of orthodontic wires frictional among ligature wire, bracket and arch wire. J Jpn Orthod Soc. 1993;52:502-8
[Google Scholar]
- Nanda RS, Ghosh J. Biomechanical considerations in sliding mechanics. In: Biomechanics in Clinical Orthodontics. Philadelphia, PA: WB Saunders Company. 188-217
[Google Scholar]
- Kusy RP, Whitley JQ. Influence of archwire and bracket dimensions on sliding mechanics: Derivations and determinations of the critical contact angles for binding. Eur J Orthod. 1999;21:199-208
[CrossRef] [PubMed] [Google Scholar]
- Kusy RP, Whitley JQ. Assessment of second-order clearances between orthodontic archwires and bracket slots via the critical contact angle for binding. Angle Orthod. 1999;69:71-80
[Google Scholar]
- Loftus BP, Ârtun J, Nicholls JI, Alonzo TA, Stoner JA. Evaluation of friction during sliding tooth movement in various bracket-archwire combinations. Am J Orthod Dentofacial Orthop. 1999;116:336-45
[CrossRef] [Google Scholar]
- Kusy RP, Whitley JQ. Resistance to sliding of orthodontic appliances in the dry and wet states: Influence of archwire alloy, interbracket distance, and bracket engagement. J Biomed Mater Res. 2000;52:797-811
[CrossRef] [Google Scholar]
- Rose CM, Zernik JH. Reduced resistance to sliding in ceramic brackets. J Clin Orthod. 1996;30:78-84
[Google Scholar]
- Mendes K, Rossouw PE. Friction: Validation of manufacturer's claim. Semin Orthod. 2003;9:236-50
[CrossRef] [Google Scholar]
- Liaw YC, Su YY, Lai YL, Lee SY. Stiffness and frictional resistance of a superelastic nickel-titanium orthodontic wire with low-stress hysteresis. Am J Orthod Dentofacial Orthop. 2007;131:578-8
[CrossRef] [PubMed] [Google Scholar] :e12-8
[CrossRef] [PubMed] [Google Scholar]
- Izuka T, Ishikawa F. Normal standards for various cephalometric analysis in Japanese adult. J Jpn Orthod Soc. 1957;16:4-12
[Google Scholar]
- Nicolls J. Frictional forces in fixed orthodontic appliances. Dent Pract Dent Rec. 1968;18:362-6
[Google Scholar]
- Ho KS, West VC. Friction: Friction resistance between edgewise brackets and archwires. Aust Orthod J. 1991;12:95-9
[Google Scholar]
- Tselepis M, Brockhurst P, West VC. The dynamic frictional resistance between orthodontic brackets and arch wires. Am J Orthod Dentofacial Orthop. 1994;106:131-8
[CrossRef] [Google Scholar]
- Ogata RH, Nanda RS, Duncanson MG, Sinha PK, Currier GF. Frictional resistances in stainless steel bracket-wire combinations with effects of vertical deflections. Am J Orthod Dentofacial Orthop. 1996;109:535-42
[CrossRef] [Google Scholar]
- Kusy RP, Whitley JQ. Friction between different wire-bracket configurations and materials. Semin Orthod. 1997;3:166-77
[CrossRef] [Google Scholar]
Show Sections
Δεν υπάρχουν σχόλια:
Δημοσίευση σχολίου